The 48yrs/F patient who visited our clinic, presented with chronic pain over the region of vertex, vAma shankha marma (lt. temple), vAma apAnga marma (near outer canthus of lt. eye), left eye ball, vAma vidhura marma (present behind the lt. ear), angle of lt. lower jaw. The patient could not identify the site of origin of pain and informed occasionally it starts from the nape of the neck and at times from the base of the head.
Concurrently she felt referred pain over the left scapular spinal area, stana rohita (the sternal angle), within glenoid cavity of shoulder and from lt. shoulder to the lateral three fingers of left hand (little, ring & middle).
Surgical history of left radical mastectomy points eight years back.
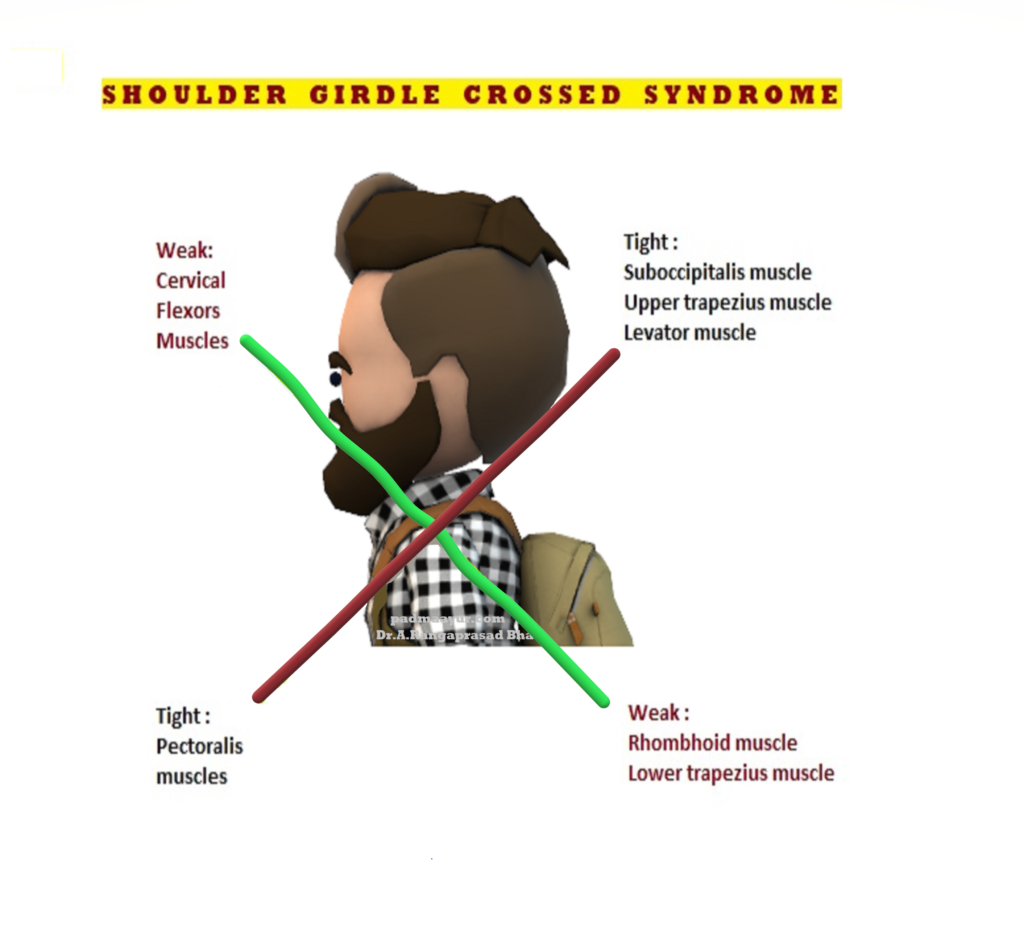
A peculiar pattern of clinical presentation, with two planes of muscle group / energy criss crossing each other were found in the patient.
The taunted upper trapezius and levator scapula on the dorsal side were seen crossing against the plane of the taunted pectoralis major and minor muscles.
Likewise the weak toned deep cervical flexors (longus colli, longus capitis etc.,) were observed crossing over the plane of middle and lower trapezius which too were weaker in tone.
The above two planes of weaker and taunted muscle groups when seen from the side of the body gives an appearance of crisscrossing as observed in a scissor.
The proximity of the shoulder as a centre point for the structures involved in above pattern and the group of symptoms involved in the clinical manifestation, yields the name “Shoulder girdle crossed syndrome”.
Applied clinical anatomy:
Clinically this sort of crisscrossing pattern of energy imbalance creates joint dysfunction specifically the particularly at the atlanto-occipital joint, the C4-C5 segment, cervicothoracic joint, glenohumeral joint, and T4-T5 segment.
When atlanto-occipital joint gets involved the chances of nerve pinching over either lesser or greater occipital nerve is a possibility presenting the manifestation of pain in the vertex, temples, eye brow, eye ball, angle of jaw and behind the ears.
The local areas of stress within the spine change the morphology neighbouring vertebrae and result in certain compromise with the normal posture. The usually observed postural changes in Shoulder girdle crossing syndrome includes forward head posture, increased cervical lordosis and thoracic kyphosis, elevated and protracted shoulders, and rotation or abduction and winging of the scapulae, depending upon the energy imbalance caused between the weaker and taunting muscles antagonistic to each other.
The glenohumeral stability may at times get decreased due to the above postural changes, as the glenoid fossa becomes more almost vertical due to weakened serratus anterior leading to abduction, rotation, and winging of the scapulae. In the event of lesser weakness of the muscle winging may not manifest but when muscle weakness is profound the winging is imminent.
Presence of pain in the region of avaTuka (nape of neck), karNa (ear), shiras (head/vertex), hanu (jaw), manyA (lateral portion of neck), bhru (eye brow) and locana (eye ball) due to the aggravation of the vAta from within and from remote areas of those body parts points towards the diagnosis of anyatovAta / अन्यतोवात explained by SushrutAcharya.
यस्यावटूकर्णशिरोहनुस्थो मन्यागतो वाऽप्यनिलोऽन्यतो वा | कुर्याद्रुजोऽति भ्रुवि लोचने वा तमन्यतोवातमुदाहरन्ति ||२७|| सुश्रुतसंहिता- उत्तरतन्त्रम् - ६. सर्वगतरोगविज्ञानीयाध्यायः || निबन्धसङ्ग्रह व्याख्या (डल्हण कृत):- अन्यतोवातमाह- यस्येत्यादि| अवटुः ग्रीवायाः पश्चिमो भागः| मन्या ग्रीवायाः पार्श्वयोः सिराविशेषः| अन्यतो वेति पृष्ठतो वेत्यर्थः| अन्यतोवात इति यथार्थेयं सञ्ज्ञा, यतोऽन्यतः स्थितो वायुरन्यतो वेदनां करोति|वातिकोऽयं साध्यश्च||२७||
The involvement of StanamUla, posterior side of neck, armpit, pectoralis, scapula & nitamba in the above case points towards the stagnation of the pranic energy in iDA nADi and that of the involvement of adhipati, sImanta, vidhura & KrukATikA points the sushumna nADi.
Marma taping along with manipulation of marma with adangal and abhyanga followed by – sthanika basti covering the regions of C2-7, T2-5, L2-S1 in periodical gap, were planned in the above case to bring back equilibrium of energy circulation within the iDa & suShumna nADis.
On the first day of treatment with manual correction of the position of the A-A joint by relaxing the krkatika marma the pain radiating to the apAnga, adhipati & vidhura got reduced in intensity.
After three days of C2-C7 sthanika vasti the pain in the following areas – occipital, vertex, around the ear, the angle of the jaw, lateral & anterior aspects of the upper neck, upper limb – got reduced completely.
The next 3 days of sthanika vasti over dorsal vertebrae showed remarkable pain reduction in the regions of kakshadhara, sthanarohita, StanamUla.
The final 3 days of sthAnika vasti over the lumbosacral controlled the pain over her lower limbs.
After 10 days of the treatment, the patient was asymptomatic and feeling energetic devoid of the fear caused by the pain of shoulder girdle syndrome / anyatovAta.
Comments are closed.