PIRIFORMIS SYNDROME MIMICKING DISC COMPRESSION PAIN
The Piriformis syndrome very often mimics the sciatic pain caused by the compression of nerve roots of sciatica by compressed discs.
Very often clinically, though the MRI findings are suggestive of disc compression, we find the cause of referral pain along the course of sciatic nerve to be the irritation of the nerve originating from underneath the piriformis muscle and not from the roots of origin of the sciatic nerve.
Many a times, due to clinical presentation of pain complained from lower back up to knee as in classical sciatica and due to such masking effect of symptom presentation the piriformis syndrome gets referred with other names like deep gluteal syndrome, wallet-sciatica, pseudo-sciatica, hip socket neuropathy, fat wallet syndrome, hip lateral rotator tendinosis, hip lateral rotator tendinitis.
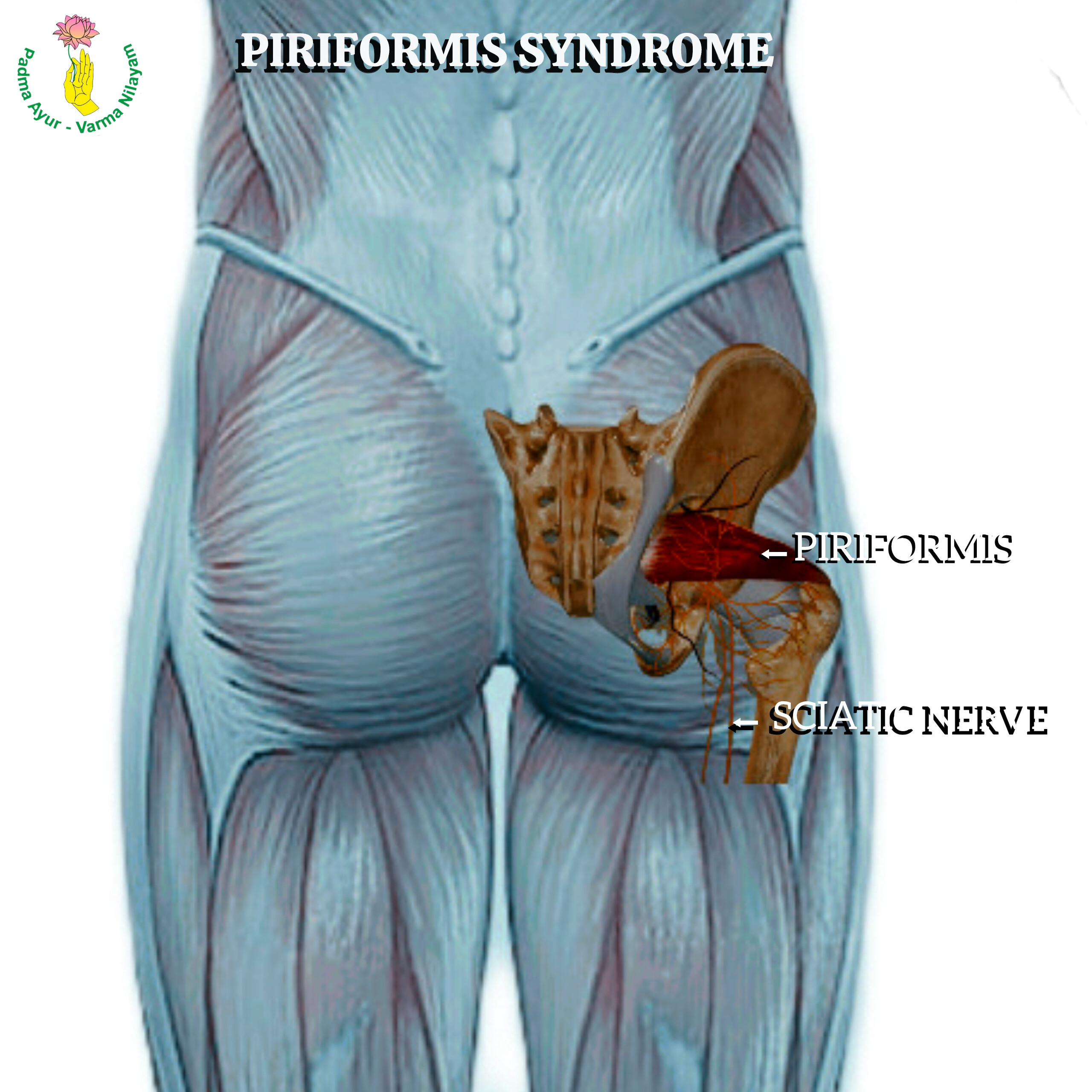
The flat, band like Piriformis muscle located in the buttocks in proximity to the hip joint, physiologically is a postural muscles which helps to maintain one’s axial posture against the gravity. Postural muscles are also referred with the names anti-gravity & tonic muscles. These muscles usually have a higher resting phase than the phasic group of muscles. The postural muscles like pyriformis usually tend towards shortness & tightness as in spasm, when excessive force is exerted over them by activities like sitting for hours together with a bulky wallet, faster climbing of staircase, dancing, running, bicycling and other such sports activities which defy the gravity.
CLINICAL SYMPTOMS: The overuse of the piriformis muscle causes an increase in the tone of the muscle at its middle causing a strong spasm resulting in compressing the sciatic nerve that which bypasses closely underneath the muscle.

The pressure thus exerted upon the sciatic nerve along its course underneath the muscle results in swelling, inflammation and exhibits symptoms of nerve irritation like tingling, burning; numbness; paraethesia or shooting pain. Physical difficulties like pain while sitting, standing, while voiding bowels.
The pain originates from the gluteal region and moves downwards through the buttock; back of the thigh; back of the leg & to reach lateral aspect of the foot. Gait gets altered and the patients starts limping when walking with compensatory external rotation of hip in want of ease from pain, which gives an impression that one of their leg is shortened.
Certain patients of wallet syndrome feel relief on lying down, upon bending their knee ar at times while walking. Certain other group of patients could find not bear the pain in any resting position but feels the comfort from the agonising pain only when they are ambulatory.
CLINICAL EXAMINATION:
Pyriformis syndrome since do not involve the nerve roots of sciatica, clinically it donot present with lower motor neuron features such as decreased deep tendon reflexes and muscular weakness in legs.
Higher Imaging investigation studies are not helpful in diagnosing the pseudo-sciatica or wallet-sciatica. The bedside clinical examinations alone comes in handy to most of the physicians.
But, the intervention and usage of MRI is helpful in identifying the underlying causes that which may not be deep gluteal syndrome, but mimics the clinical presentation of it and thus help in differential diagnosing some of the following clinical or surgical conditions like – Herniated intervertebral disc, osteo arthritis of hip, lumbosacral radiculopathy, sacro iliac joint disease, lumbar spinal stenosis, femoro-acetabular impingement, renal stones, tumours and cysts in gluteal region, appendicitis, prostate disorders, malignancy conditions in pelvic organs, pseudo-aneurysm in inferior gluteal artery etc.,
When clinically examined by palpating over the muscle belly of the piriformis muscle or over the greater sciatic notch it is possible to detect the muscle spasm. A little bit deeper palpation over the retro trochanteric area tenderness when elicited one can observe the increase in the numbness of the leg and tightness of the thigh muscles.
The straight leg test when done passively by the patient himself pain gets felt.
The Frieberg sign is observed to be positive, when the patient passively rotates his hip internally by lying in supine position, as caused by the pressure of sciatic nerve at the sacrospinous ligament.
The painful flexion; adduction & internal rotation confirms the positive Fair sign, reconfirming the Piriformis syndrome clinically.
AYURVEDA & MARMA CHIKITSA MANAGEMENT:
While treating this māmsa gata vāta condition caused by Āghāta (indirect injury) the gati of the individual māmsa peśi like prasarana, Ākuñcana; the extent of Āghāta, the nature of vedana and karma hāni etc are considered in selecting the appropriate therapeutic needs in addressing the condition.
Accordingly, upanāha, sthānika picu, piṇdasveda or nādi sveda are done if the roga bala is avara to madhyama.
But in case if the roga bala is pravara due to the involvement of the muscle fascia (māmsa peśi) prapīḍana of the appropriate marmas around the the sphik, ūru & pṛṣṭha deśa along with application of vastrapaṭṭika over the affected māmsa-tantus help the patient recover from the pain. It needs to be understood that any particular peśi is in samavāya saṃbandha with another peśi through the interluding muscle fascia. And that when one layer of the peśi is pulled in any one particular spot over it, pressure of pull gets transferred to the underlying peśi through the fascia and thus depending upon the pull caused by the stretching with the vastra paṭṭika , the pressure exerted reaches layers deep within the area of its application. Thus, any existing bio-energy stagnation in the marmās present underneath the structure governing its karma, gets released by the indirect action of effleurage caused by the vastrapaṭṭika from outside through the stretch receptors of the skin & muscles which occurs at the momentary kinesis of the muscles during the locomotion of the patient.
Internally medicines with vātānulomaka, vedanāhara & āvaraṇahara therapeutic actions are helpful.
GLOSSARY OF AYURVEDA TERMS USED IN THE ARTICLE:
māmsa gata vāta – vata localised in muscles
māmsa peśi – muscle tendon or fascia
prasarana – stretching
Ākuñcana – contraction
Āghāta – injury
gati – motion
upanāha – poultice
sthānika picu – local application of a cotton dipped with oil
piṇdasveda – a method of inducing localised sudation using a bolus prepared with herbal leaves
nādi sveda – a method of inducing localised sudation using a hollow tube.
roga bala – intensity of disease
avara – milder
madhyama – moderate
pravara roga bala – severe intensity of disease
prapīḍana – application of pressure or squeezing
marma – vital point or vulnerable point or concealed point present in human body.
sphik – waist
ūru – thigh
pṛṣṭha – lower back
māmsa-tantu – muscle fibre or fascia
samavāya saṃbandha – intimate & constant connection
vastra paṭṭika – adhsesive cloth tape
vātānulomaka – movement of vAta in it’s due course of intended direction
vedanāhara – anodyne or pain reliever
āvaraṇahara – displacing and eliminating the concealed or obstructed vAta dosha ,over its intended pathway, either by other 2 doShAs; 7 dhAtus or 3 malAs.
Comments are closed.